Episode Details
Back to Episodes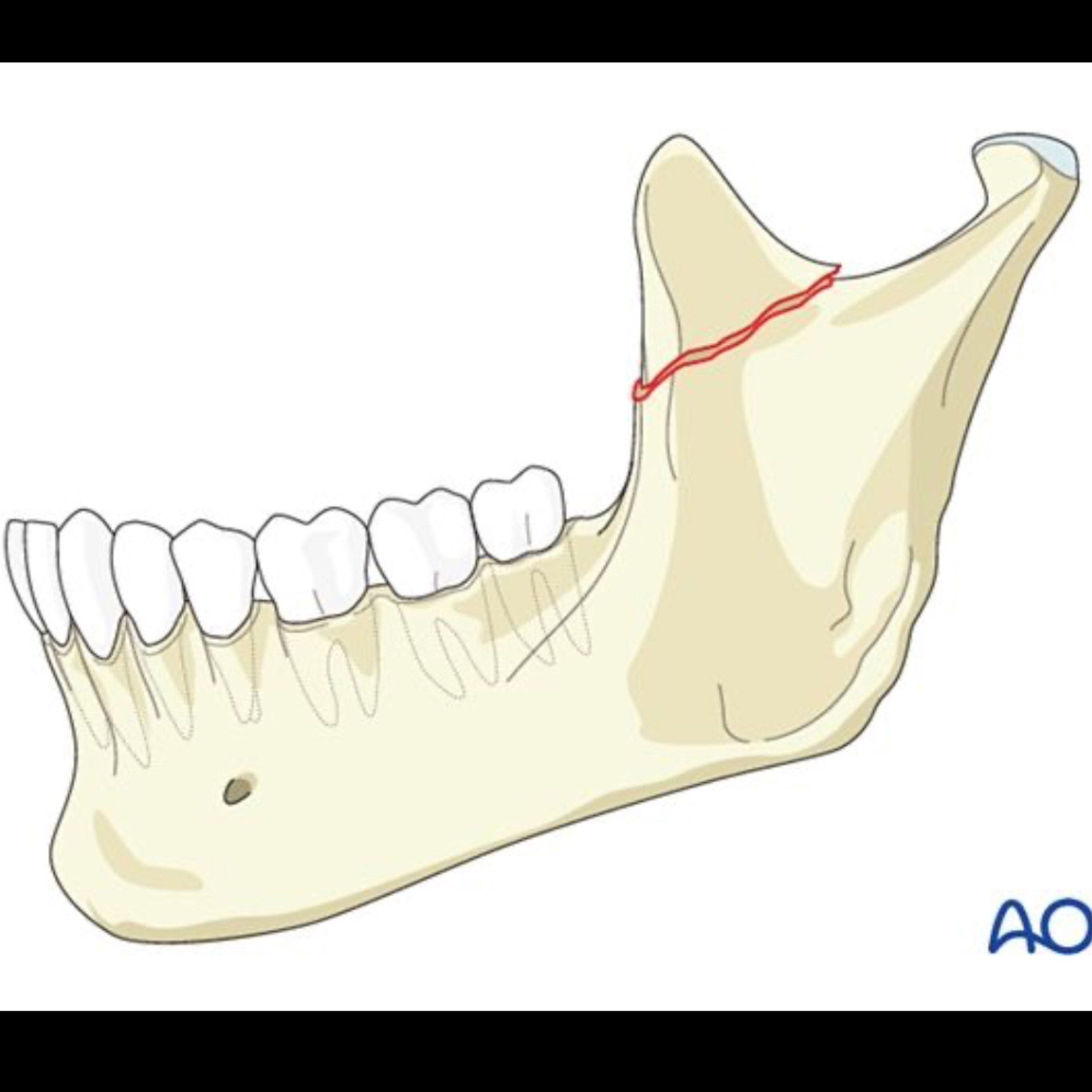
📝 “What is the Coronoidectomy via Intraoral Approach?”
Description
Quick Review #268 - #surgery #surgeon #doctorgallagher #oralsurgery #oralsurgeon #omfs #dentist #dentistry #dental #coronoidectomy
2.26.25
Indications:
• Coronoid process hyperplasia
• Trismus secondary to coronoid impingement (e.g., post-traumatic ankylosis, temporalis muscle hyperactivity)
• Access to zygomatic arch fractures
Surgical Steps
1. Preoperative Considerations
• Assess mouth opening and obtain preoperative imaging (CT scan preferred).
• Consider IV steroids to reduce postoperative edema.
2. Anesthesia and Patient Positioning
• General anesthesia with nasal intubation to maximize intraoral access.
• Head tilted slightly toward the contralateral side.
3. Intraoral Incision and Exposure
• Use a mouth prop to maintain jaw opening.
• A mucosal incision is made over the anterior border of the ramus, extending superiorly into the maxillary vestibule.
• Subperiosteal dissection exposes the coronoid process, preserving the buccal fat pad to minimize fibrosis.
• Retract the temporalis muscle superiorly to visualize the coronoid.
4. Osteotomy and Removal of the Coronoid Process
• Identify the coronoid process and ensure adequate exposure.
• Use a reciprocating saw or osteotome to perform an osteotomy at the coronoid base, just superior to the sigmoid notch.
• Remove the coronoid segment with forceps, taking care to avoid excessive traction on the temporalis.
• If necessary, additional bone resection may be performed to improve range of motion.
5. Hemostasis and Closure
• Irrigate the site thoroughly to remove bone debris.
• Achieve hemostasis with electrocautery or hemostatic agents.
• Close the mucosal incision with absorbable sutures.
Pearls
* Adequate exposure – Proper subperiosteal dissection minimizes bleeding and facilitates visualization.
* Preserve mucosal integrity – Avoid excessive stripping of periosteum to reduce fibrosis risk.
* Controlled osteotomy – Use a reciprocating saw for a precise cut to avoid unnecessary trauma.
* Immediate mobilization – Early physiotherapy prevents postoperative fibrosis and ankylosis.
* Hemostasis – Cauterization of the pterygoid venous plexus minimizes bleeding.
Pitfalls
* Inadequate exposure – Poor visualization increases risk of damaging the temporalis muscle.
* Excessive traction on the temporalis – May lead to postoperative pain and muscle dysfunction.
* Injury to maxillary artery branches – Risk of excessive bleeding if deep dissection is not controlled.
* Failure to initiate early physiotherapy – Can result in trismus and scar formation.
* Over-resection – Removing excessive bone can weaken the mandible structurally.
References:
1. Ellis, E. III, & Schubert, W. (n.d.). Coronoid process fractures. AO Surgery Reference.
2. Roy, T., & Reid, R. (2021). A novel approach to coronoidectomy: The modified Keen technique. Journal of Craniofacial Surgery, 32(3), 1150-1151.
3. ChatGPT. 2025
#podcast #dentalpodcast #doctorgallagherpodcast #doctorgallagherspodcast #doctor #dentist #dentistry #oralsurgery #dental #dentalschool #dentalstudent #doctorlife #dentistlife #oralsurgeon #doctorgallagher