Episode Details
Back to Episodes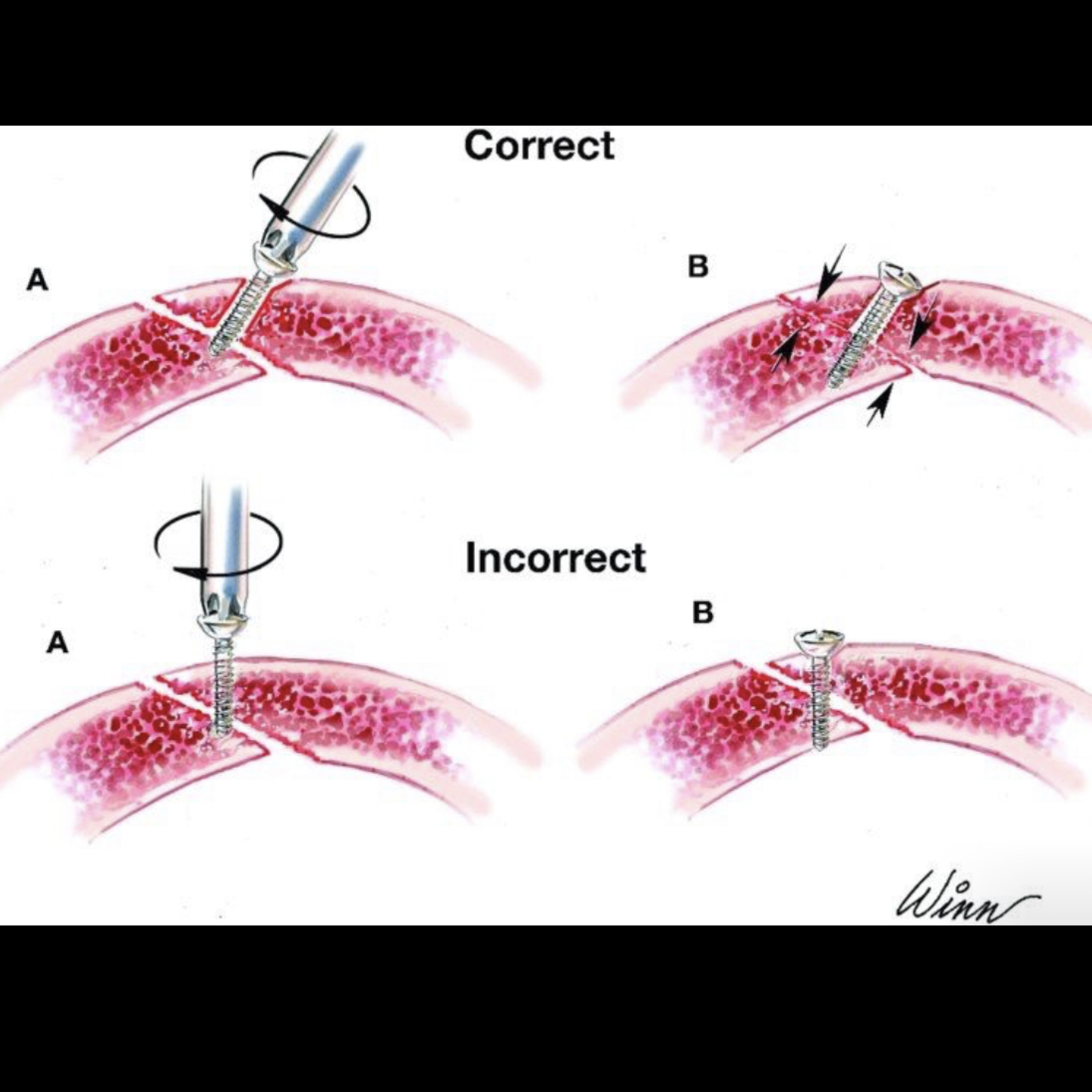
📝 “What is the Lag Screw Technique for Mandible Fractures?”
Description
- 11.26.24
Quick Review #256 - #surgery #surgeon #doctorgallagher #oralsurgery #oralsurgeon #omfs #dentist #dentistry #dental #lagscrew #trauma #facialtrauma
The lag screw technique is a specialized method of open reduction and internal fixation (ORIF) used for mandibular fractures, particularly symphysis and parasymphysis fractures. It utilizes cortical lag screws to achieve interfragmentary compression, which stabilizes the fracture while maintaining proper anatomical alignment.
Key Concepts of the Lag Screw Technique
1. Principle of Lag Screw Fixation:
• The lag screw is inserted obliquely across the fracture line so that it compresses the bone fragments together as it is tightened.
• A gliding hole is drilled in the near cortex, allowing the screw head to pass freely without engaging the bone.
• A smaller-diameter thread hole is drilled in the far cortex, ensuring the threads engage only the far cortex, pulling the two fragments together.
2. Indications:
• Simple fractures of the symphysis or parasymphysis.
• Fractures with minimal comminution or fragmentation.
• Cases where minimal hardware is desired (e.g., reducing implant load in younger patients).
3. Surgical Steps:
• Expose the fracture site via an intraoral or extraoral approach, depending on accessibility and surgeon preference.
• Reduce the fracture anatomically and maintain the reduction using temporary fixation (e.g., wire or bone clamp).
• Drill the gliding hole through the near cortex.
• Drill the thread hole through the far cortex.
• Insert the lag screw and tighten it to compress the fracture line.
4. Biomechanical Advantage:
• Creates direct compression across the fracture line, leading to primary bone healing without the need for callus formation.
• Can be used as a standalone fixation or in conjunction with other stabilization methods, such as plates or arch bars.
Key Pitfalls to Avoid
1. Improper Screw Placement:
• The screw must be inserted obliquely to cross the fracture at a right angle to the fracture line. Incorrect angulation can lead to inadequate compression or fragment displacement.
2. Over-Tightening:
• Excessive tightening of the screw can lead to fracture fragment rotation or crushing of the cortical bone, compromising the fixation.
3. Failure to Drill Proper Holes:
• Failing to create a gliding hole in the near cortex will result in both cortices engaging the threads, preventing compression.
References:
1. Haggerty, C. J. (n.d.). Chapter 13: Mandibular fractures. In Pocket Dentistry.
2. Ellis, E., & Zide, M. F. (2006). Surgical Approaches to the Facial Skeleton (2nd ed.). Lippincott Williams & Wilkins.
3. Miloro, M., Ghali, G. E., Larsen, P. E., & Waite, P. (Eds.). (2022). Peterson’s Principles of Oral and Maxillofacial Surgery (4th ed.). Springer.
4. ChatGPT.2024
#podcast #podcasts #dentalpodcast #dentalpodcasts #doctorgallagherpodcast #doctorgallagherspodcast #doctor #dentistry #oralsurgery #dental #viral #dentalschool #dentalstudent #omfs #surgeon #doctorlife #dentistlife #residency #oralsurgeon #dentist #doctorgallagher